If you are interested in longevity, you understand that disease prevention is one of the most important elements.
Cardiovascular disease is the number one killer worldwide, and high cholesterol is one of the greatest risk factors.
But unfortunately, most doctors are not up on the current literature when it comes to cholesterol.
The standard practice for predicting cardiovascular risk has been to measure LDL cholesterol.
Everyone knows the saying, “LDL is the bad cholesterol.”
But recently, it has been discovered that apoB actually captures the full picture of atherogenic risk.
If you ask most people what apoB is, they don’t have the slightest clue.
And neither do their physicians.
But let me explain what apoB is and why it is the preferred metric for assessing cardiovascular risk.
Before I can explain what apoB is, you need to understand cholesterol first.
What is Cholesterol?
Cholesterol is an essential lipid used by your body to make hormones and, most importantly, the cell membrane in every cell of your body.
Without cholesterol, we would have no life.
It is such an important molecule.
But cholesterol is a lipid.
And lipids are hydrophobic, meaning that they don’t dissolve in water.
This presents a problem because your blood plasma is primarily made of water.
And your plasma is the fluid that circulates substances throughout your body.
It’s the water to the channel, so to speak.
But water and fats don’t mix, as you know.
And since cholesterol is a fat, it can’t be dissolved in your blood plasma.
So your body needs a way to traffic this cholesterol.
And this trafficking molecule is called a lipoprotein.
What are Lipoproteins?
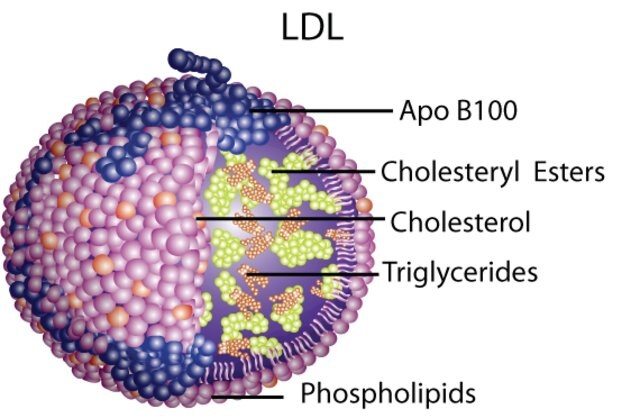
Lipoproteins are spherical structures that contain cholesterol and triglycerides.
Triglycerides are a form of fatty acids that make up the bulk of your body’s fat stores.
Lipoproteins are used to transport cholesterol and triglycerides.
They come in a couple of different families, which do different things in the body.
The APOA lipoprotein family defines the HDL particles.
But we won’t be going into HDL particles in this article.
The APOB family is really what we want to discuss.
The APOB family includes:
These particles go from largest to smallest, as shown in this figure.
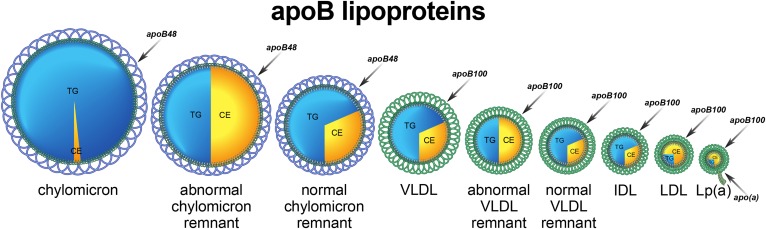
You will also notice that chylomicrons contain the most triglyceride, whereas LDL particles contain the least.
As these particles are trafficked throughout your body, they are converted into one another as they drop off their triglyceride-rich core to the appropriate adipocytes.
The biochemistry of it gets complicated, but just understand that VLDLs become IDLs which eventually become LDLs.
And this is because they slowly get rid of their triglyceride.
The LDL particle becomes the most cholesterol rich particle.
And these are the particles which are “bad” because they deliver cholesterol to the artery wall.
Cholesterol Measurements
When you get a cholesterol panel, they will likely give you three measurements.
1.) Total cholesterol
2.) LDL cholesterol
3.) HDL cholesterol
All three of these are measured as a concentration.
So for total cholesterol, if they crushed up all of the cholesterol-containing lipoproteins and measured the concentration, it would be the number you get on your panel represented like this:
Total Cholesterol = 100mg/dL
100mg of cholesterol in 1dL of your blood plasma.
Total Cholesterol and LDL cholesterol are the current standard used to measure cardiovascular risk.
Cholesterol History

In the 1950’s Ancel Keys was one of the first people to measure total plasma cholesterol, and it became known that high cholesterol was associated with an increased risk of cardiovascular disease.
15 years later, Fredrickson, Levy, Lees, and other scientists fractionated the lipoproteins and realized that there are different versions (VLDL, LDL, HDL, etc).
Later it became known that there were two families of LDL particles.
APOA and APOB.
Is LDL Cholesterol Enough?
So, LDL-C is associated with risk.
This is well established in the guidelines.
But is it enough?
Perhaps for some people.
But what if you have two people who have an LDL-C of 100mg/dL.
One has a lot of smaller LDL particles.
And the other has fewer, larger particles.
To have the same total cholesterol concentration, the person with the smaller particles needs MORE of them.
And here is where we get to the crux of the matter.
More Particles = More Risk
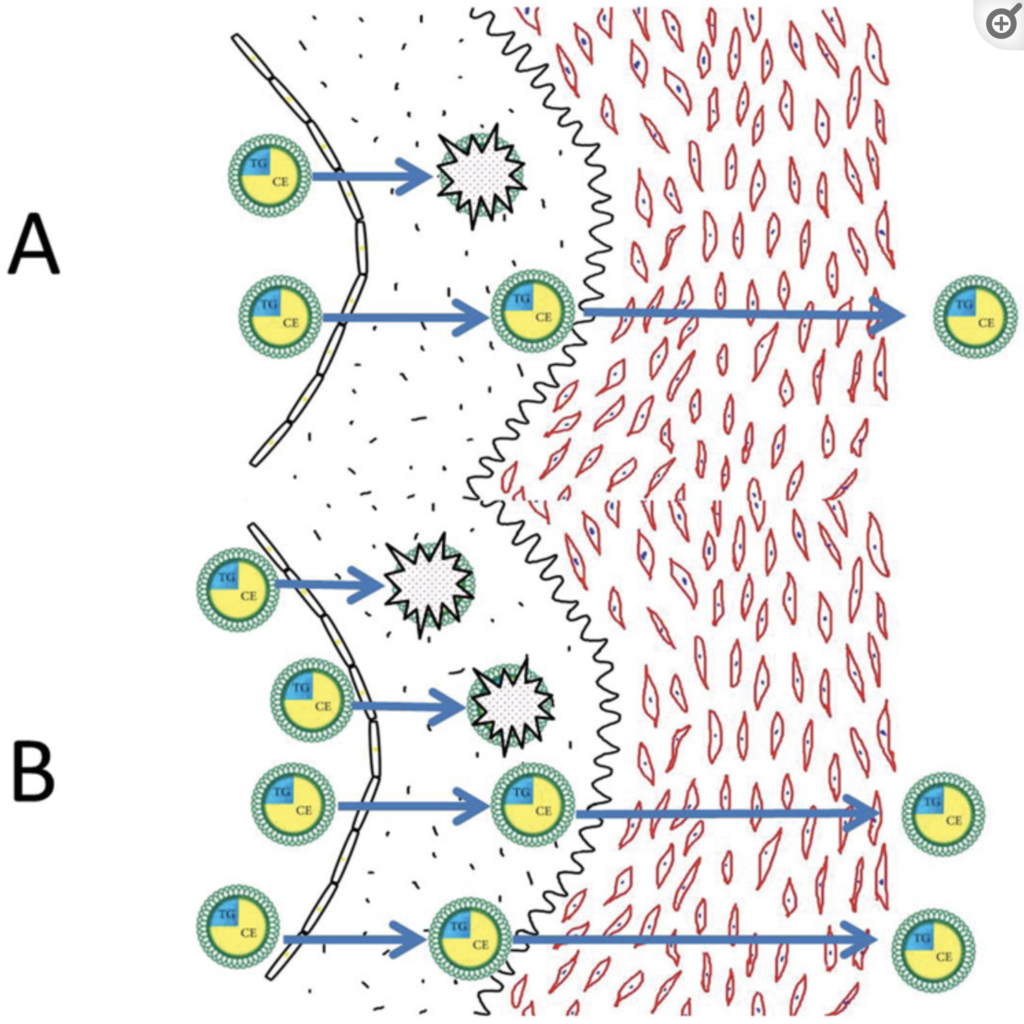
Particle number is a better predictor or risk than concentration alone.
Why?
Because the more LDL particles you have, the more chances there are to get stuck within the subendothelial space and become oxidized.
This is what causes heart disease, bottom line.
LDL particles get stuck in the artery and become oxidized.
This then leads to a cascade of inflammatory events that leads to plaque accumulation and, eventually, a plaque rupture.
The plaque rupture is what causes a heart attack.
So – particle number matters.
Why ApoB is the Best Metric
Measuring apoB is the preferred metric because it is a proxy for particle number.
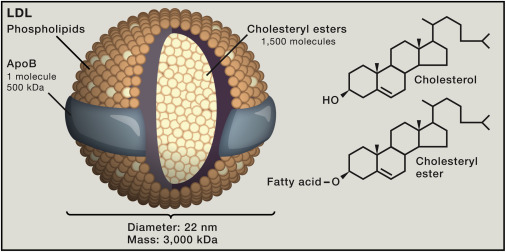
You can think of apoB as the signature protein on an LDL particle.
There is only one apoB signature protein per LDL particle.
Regardless of density, an apoB assay detects the presence of these atherogenic particles, in contrast to LDL cholesterol alone.
Because remember, LDL-C is a concentration.
Concentration is mass/volume.
It says nothing about particle number.
So when it comes to your cholesterol panel, there is a gradation in how refined each metric is at assessing risk.
Total Cholesterol – Not refined
LDL Cholesterol – A little more refined
Non-HDL – More refined
ApoB – Really refined!
Unfortunately, most doctors don’t have time to read the current literature and are way behind when it comes to cholesterol.
The Evidence Has Mounted
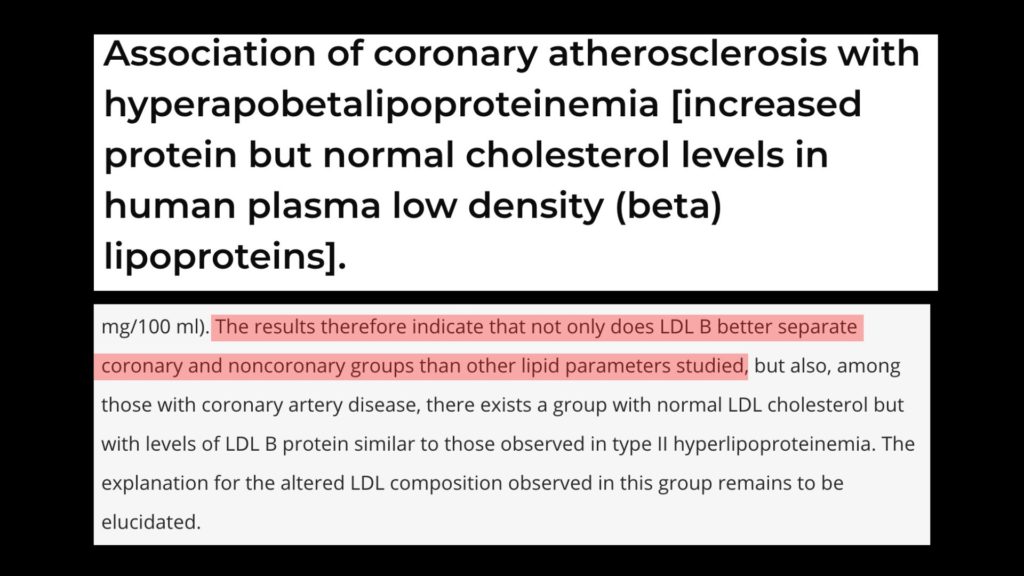
A groundbreaking paper was published in 1980 by Sniderman that described the significance of cholesterol particle number compared to cholesterol concentration.
They used coronary angiography to compare people with clean coronaries to people with diseased coronaries.
The findings were remarkable.
There was a little difference in triglyceride.
A small difference in cholesterol.
But a marked difference in apoB.
Additionally, there was also a group with diseased arteries in the study that had normal LDL cholesterol but high levels of apoB.
These findings lend credence to apoB as the preferred metric of assessing risk.
Even More Evidence for ApoB?
Since this paper has been published, there have been many more studies published confirming that apoB reigns superior.
A more recent paper showed the risk of myocardial infarction in patients with and without atherosclerosis is best predicted by the number of apoB particles.
This risk is definitively independent of both the lipid content and the type of lipoproteins typically measured.
According to the lead investigator:
“We looked at apolipoprotein B, non-HDL cholesterol, and triglycerides, and all three are predictive of risk when you look at them independently and without adjustment. However, when you also adjusted for the other lipid parameters, apolipoprotein B was the only one that remained significant.”
Sniderman and Colleagues then published a follow-up slam dunk paper about the findings.
“The debate is over,” to quote Sniderman.
What to Ask Your Doctor

So, the next time you go to the doctor, ask them to measure your apoB.
You can cite the literature presented in this article if they don’t know what you are talking about.
And don’t be surprised if they look at you like you have two heads.
Unfortunately a lot of docs are not up on the current lipid literature.
Longevity & Prevention

Living a long, healthy life is all about disease prevention.
You want to delay the onset of the diseases which carry the most mortality risk.
I have written extensively about these disease processes.
They are cardiovascular disease, cancer, and neurodegeneration.
It’s imperative to begin a prevention strategy as soon as possible, no matter how old you are.
But if you are in your middle-aged years, it is especially important.
Age is a risk factor for all three of these diseases, and you may have already begun noticing some changes to your health.
High cholesterol, high blood pressure, high blood sugar, decreased muscle mass, increased body fat.
These are just a few of the common changes middle-aged individuals begin to experience.
If you need help getting back on track with your health & fitness, take a look at my coaching options.
I have helped hundreds of middle-aged individuals reclaim their health through comprehensive lifestyle interventions.
Send me an email, and we can begin discussing a plan of action.
I will coach you each step of the way.