It’s common knowledge that heart disease most prominently afflicts the middle-aged population.
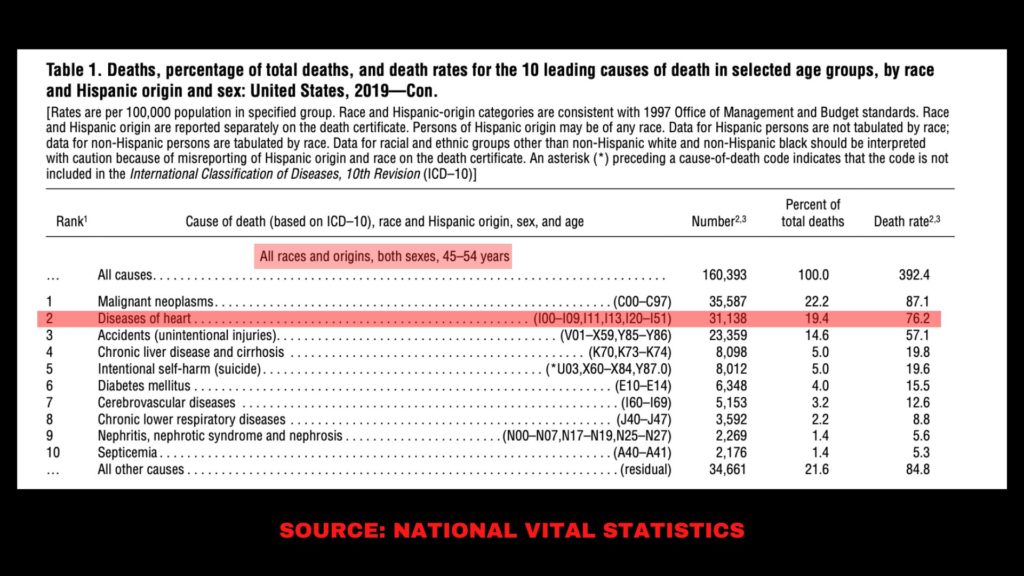
Between the fourth and fifth decade of life, cardiovascular related death ranks #2 across all races and in both sexes.
But as I have written about before, the disease process starts well before the manifestation of symptoms.
It would be comical to assume that a heart attack is the first presentation of atherosclerotic dysfunction.
In fact, in this article you will learn that cardiovascular disease begins as early as the FIRST decade of life.
That’s right, when you are 10 years old the process is already underway.
We will get into the nuanced discussion of disease classification and its true clinical significance but the point is this.
Heart disease is a lifelong progressive process and the best thing you can do to mitigate risk is to arm yourself with knowledge first and then implement prevention strategies so that you don’t become another statistic during your middle-aged years.
Much of my work focuses on improving the metabolic health of my clients’ during their middle-aged years when the phenotype of disease manifestation most commonly begins (insulin resistance, dyslipidemia, hypertension, obesity, etc).
Let’s take a look at some of the poignant evidence for the manifestation of cardiovascular disease by lesion classification and how you can get ahead of your risk for cardiovascular insult.
The Groundbreaking Work of Stary and Colleagues

I can think of no better scientific literature to cite than the work from Herbert Stary and colleagues as it relates to the early manifestation of cardiovascular disease and its progression.
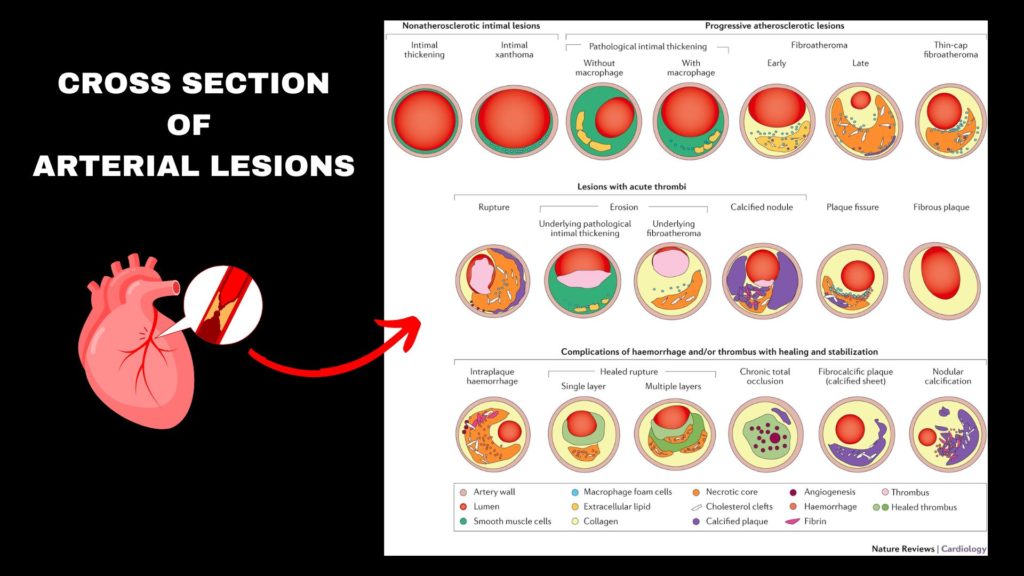
In 1995 Stary and colleagues published a series of papers which served to classify various atherosclerotic lesions based on their histology.
In layman terms, they came up with a classification system by which to define the various types of arterial disease states by their morphology.
This work became pinnacle to the understanding of the atherosclerotic disease process.
His work is fundamental to any cardiologist and while I am not a physician, his work too has impacted the way I think about heart disease.
Atherosclerotic Lesions
Atherosclerotic lesions are basically abnormal growths on the artery wall which ultimately lead to the final event in the heart disease process – that of an ischemic event (i.e. blood occlusion which leads to a lack of oxygenation in the heart tissue and the associated damage).
Most commonly known as a heart attack and/or stroke.
You might already know that lipids have something to do with the heart disease process.
That is, cholesterol ending up in places where it shouldn’t be like the artery wall.
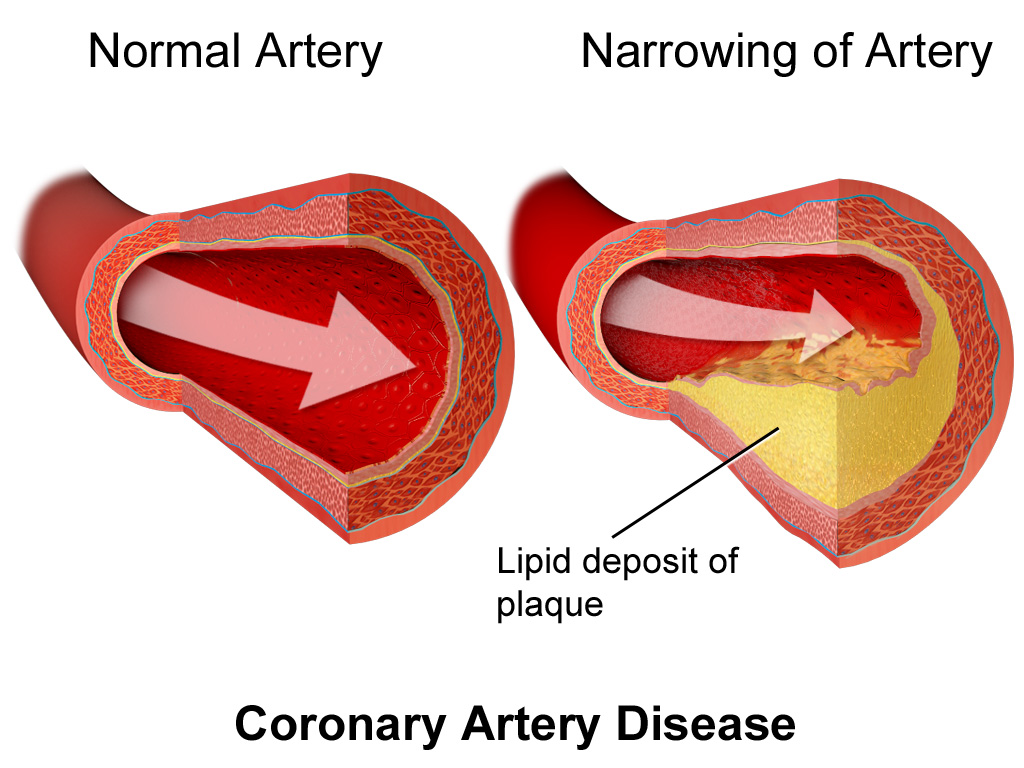
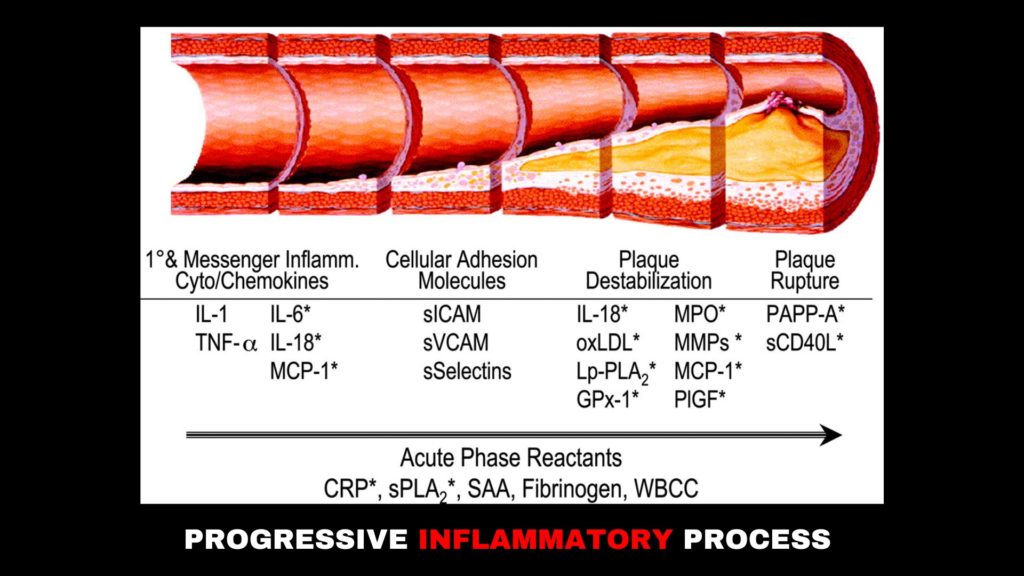
Eventually the accumulation of lipids in the artery wall leads to a cascade of events by which the body tries to repair the damage caused by lipid accumulation.
This leads to more oxidative stress and the formation of what is commonly referred to as plaque.
This plaque eventually ruptures and causes the clinical event that we all know as a heart attack or stroke.
Type 1 Lesions
By the time that arterial lesions are advanced enough to cause clinical symptoms, it is often too late.
The reality is, these lesions have to start somewhere, and this type of lesion is called the type 1 lesion.
And guess what, it starts during the first decade of life!
That’s right, between birth and age ten!
It sounds hard to believe, but the heart disease process starts incredibly early.
And while type 1 lesions are far from clinically significant, it displays that the heart disease process is a long progressive process and warrants a long term view of risk profile.
To quote Stary:
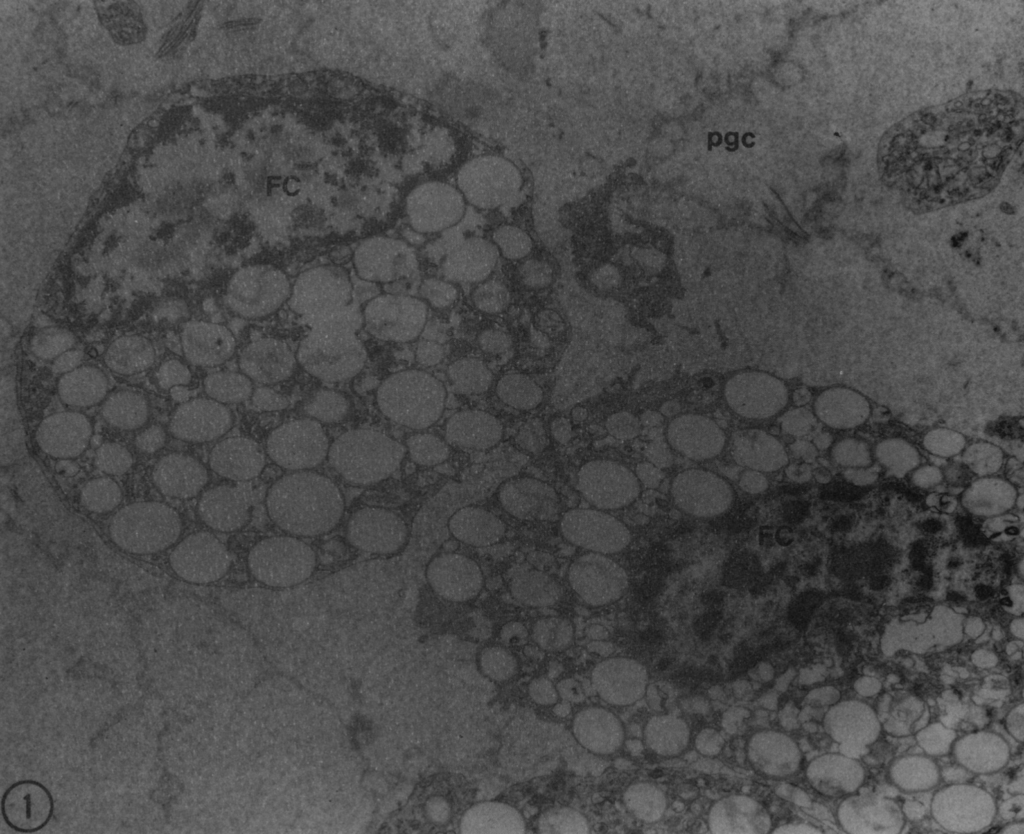
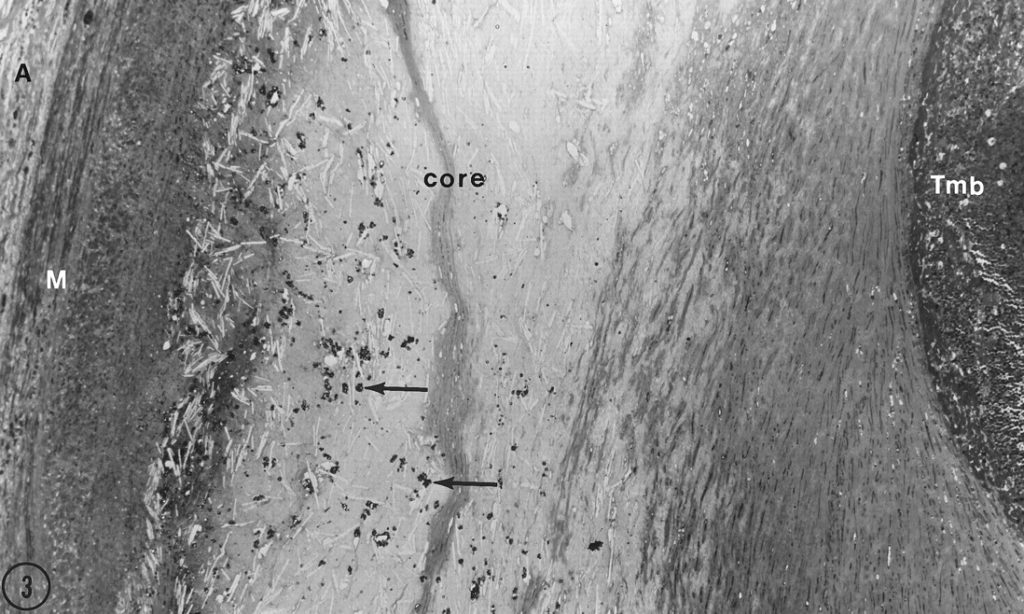
“The initial histological changes in the human intima are minimal. Small, isolated groups of macrophages containing lipid droplets (macrophage foam cells) form. In coronary arteries these cells preferentially accumulate in regions of the intima that have an adaptive intimal thickening of the eccentric type. These locations are identical to those in which type II lesions are more prominent and in which type III or advanced lesions develop first in young adults if such lesions develop at all. In the first 8 months of life, 45% of infants have macrophage foam cells in their coronary arteries and macrophages without lipid droplets are increased twofold above normal.”
To put this into context, Stary is saying that although we would never consider an infant to be clinically at risk for cardiovascular complications, the initial development of cardiovascular insult begins in fact, during infancy.
You can see a photo above which displays the start of a type 1 lesion in an infant.
The location of these initial changes in the infant’s artery are the same as those who present with clinically significant lesions during their adulthood!
Unfortunately, the current medical establishment only looks at a 10-year risk profile.
But if we change our frame to thinking of this disease as a lifelong process, then I believe the urgency for preventative measures will be made ever more apparent.
Lesion Type and Middle-Age
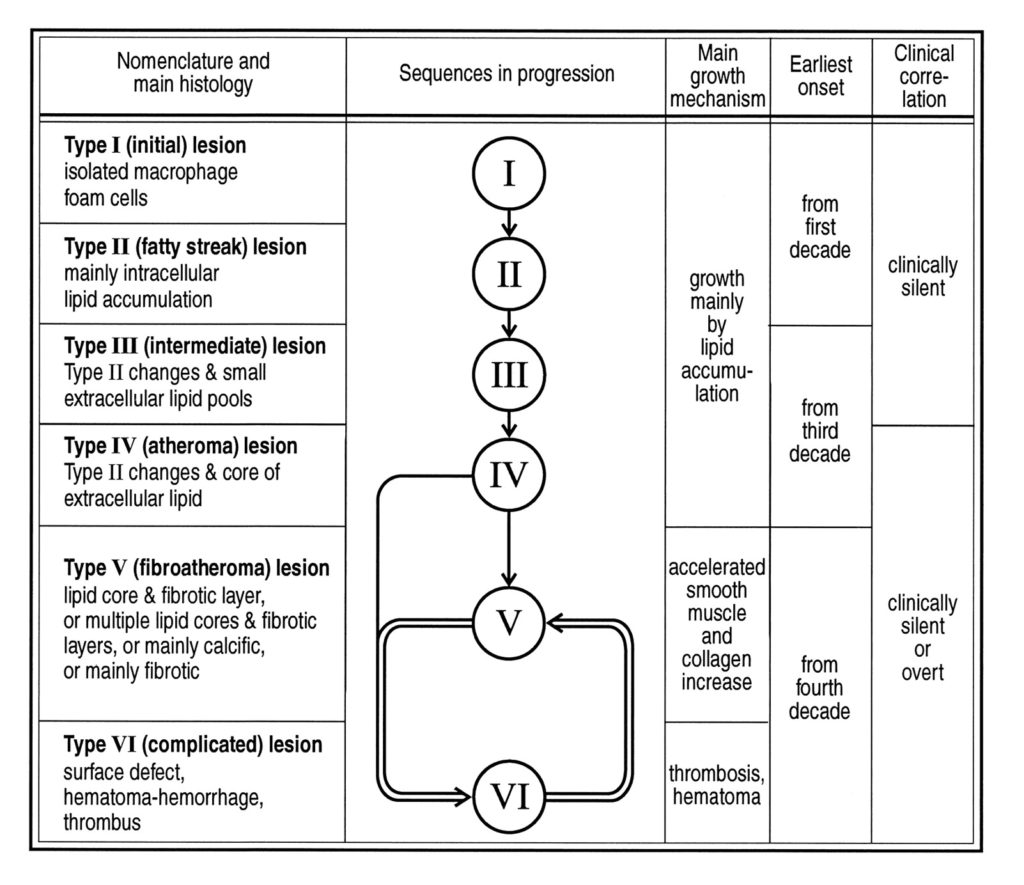
Stary discusses the progression of these arterial lesions and gives them subsequent classifications (one through six)
During middle-age is when we mostly commonly see the prevalence of type six, the most advanced and dangerous type.
By this point, the lesion has advanced to become calcific by nature with a strong lipid core and displays evidence of a hematoma.
Ripe and ready to rupture.
And this is precisely why we see the rise of cardiovascular death around the fourth decade of life and progressive rises thereafter.
Now you understand that the lesions which ended in a heart attack or stroke did not come out of the blue.
The work by Stary and Colleagues clearly shows that these lesions are progressive, and progressive over an incredibly long period of time.
If you are middle-aged, you already hold the greatest risk of cardiovascular insult.
And while not everyone dies FROM heart disease, everyone will die WITH some degree of it.
But as morbid as this sounds, there is a beacon of light at the end of the tunnel.

Prevention

And this comes down to prevention.
The best thing that you can do to reduce your mortality risk from cardiovascular disease is to exercise!
Specifically, aerobic exercise.
I have written extensively about this topic, but it has been well established that aerobic exercise reduces all cause mortality significantly and has a direct impact on preventing cardiovascular disease.
The bottom line is that your endothelial health is at the root of your cardiovascular disease risk.
And aerobic exercise is a powerful tool for improving your endothelial health.
I cannot stress the importance of implementing a plan of action, especially during your middle-aged years.
Take a look at the various articles I have written and begin your prevention strategy today.
I’d also be happy to answer any questions you have and get you started.
You can also take a look at my coaching opportunities.
I look forward to hearing from you!